
This retrospective observational study encompassed all consecutive FSEx conducted by the Center for Research and Training in Disaster Medicine, Humanitarian Aid, and Global Health (CRIMEDIM; Università del Piemonte Orientale; Novara, Italy) within its institutional activity over ten years (from January 2012 to December 2022).
Exercise design
All FSEx were designed and executed in a uniform and standardized manner. Each incorporated a storyboard that outlined a predetermined number of casualties. The severity and distribution of these casualties were established based on epidemiological reports, with the objective to closely resemble the characteristics of the targeted event. Once epidemiological profiles were defined, specific sets of simulated casualties were generated accordingly. Casualty sets comprised three components: (i) paper Dynamic Casualty Cards (DCCs), which featured evolving vital signs and were designed to be placed into transparent plastic envelopes and safely attached to a lanyard to be worn around the casualty neck; (ii) instructions for casualties ‘moulage’, providing professional guidance on creating a standard and high-fidelity wounds on the actors for a realistic appearance and (iii) storyboards for simulating realistic and evolving patients, serving as guidelines to match the data cards and simulate injuries and associated symptoms. All simulated casualties underwent standardized training on how to progress according to the provided storyboard, passing time and receiving treatments. The instructions given to participants in delivering treatments to simulated victims were: (i) to place the necessary treatment devices (e.g., fluids, medications) near the victim; (ii) to communicate the administration of the treatment; (iii) to remain in close proximity to the victim for a duration realistically corresponding to the treatment time. DCCs featured all necessary vitals required for assigning triage codes based on the START system. Based on these vitals, each casualty had a predetermined expected (correct) triage code. In addition to their role as casualties, participants also collected data by documenting their assigned triage codes at the scene and upon arrival at the hospital, as well as key timestamps during the exercise, including time to triage, time to a prehospital staging area, and time to prehospital scene exit. All these times were measured from the start of the exercise. These data are then computed and used in the after-action debriefing. Details about the casualty evolution method, general structure of the simulation, and DCCs were described in a series of previous papers. [16, 18,19,20,21,22,23,24] An example of DCCs is presented in Additional file 1: Fig. 1S.
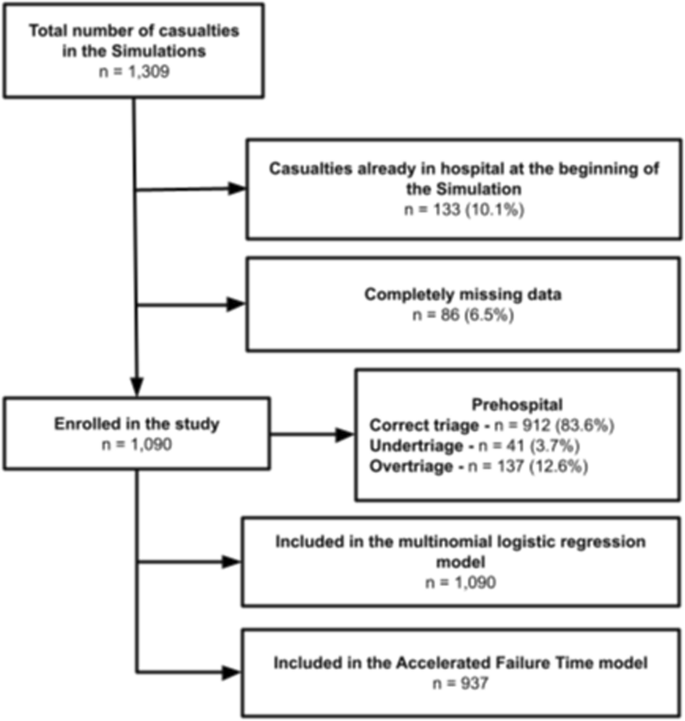
Flowchart of simulated casualties in the study
Inclusion and exclusion criteria
To be enrolled in the study, each FSEx had to incorporate at least one prehospital scenario and at least one simulated hospital. The analysis excluded all casualties specifically designated to be observed only at the hospital and did not undergo prehospital triage.
Data collection
For each FSEx, the master database including pre-existing exercise-specific casualty profiles, expected and assigned triage codes, and key management times, was thoroughly reviewed and consolidated into a single file for analysis.
Included variables consisted of:
-
Exercise and casualty-related data—exercise unique identification number, simulated casualty unique identification number, expected prehospital first triage following the START algorithm, assigned prehospital and hospital triage.
-
DCC simulated vital parameters—heart rate, systolic blood pressure, blood oxygen saturation, level of consciousness (AVPU scale)
-
Simulated anatomical injuries—pre-defined casualty injury severity score (ISS), pre-defined abbreviated injury scales (AIS).
-
Scenario management times—time-to-triage, time to Collecting Area, Time from Triage to Scene Departure, Prehospital Scene Time, Time to Hospital, Time to final disposition.
-
Experience of the group of rescuers—Exercises managed by trained professionals completing a Master of Science in Disaster Medicine (European master in disaster medicine, EMDM,) [25] were arbitrarily classified as “expert”, while exercises managed by junior doctors or trainees who completed a basic course in disaster medicine were classified as “non-expert”. This classification is based on our previous work [16].
Statistical analysis
Casualties were grouped into three categories: correct triage, overtriage, and undertriage, based on how the assigned triage matched the expected one.
Continuous variables were represented as either medians and interquartile ranges (IQR) or means and standard deviations, depending on their distribution assessed with QQ plots. The Kruskal–Wallis test or one-way analysis of variance was used to compare these variables as needed. Categorical variables were presented as counts and percentages, and the Chi-square test or Fisher’s exact test was used for comparison when suitable.
A multinomial logistic regression model was constructed to examine the impact of various physiological and anatomical factors on the risk of overtriage or undertriage in prehospital settings. In this model, triage evaluation was the dependent variable, with correct triage serving as the reference outcome. The effects of individual factors under investigation were expressed as relative risk ratios (RRR).
Vital parameters, Injury Severity Score (ISS), Abbreviated Injury Scale (AIS) scores, and the experience of the operators were tested as independent variables in the model. A stepwise forward and backward selection of variables was performed based on the Akaike Information Criterion (AIC).
For the secondary objective, the time from triage to exit was used. This metric was considered less influenced by the spatial distribution of casualties within the scenario and the rescue teams’ exploration path. A survival analysis approach was adopted to investigate factors influencing the triage-to-exit time.
The full model, which included anatomical lesions, physiological parameters, the group’s experience, and observed triage as independent covariates, fit a Weibull distribution well (Additional file 1: Fig. 2S). However, the assumption of proportional hazards was not met. As a result, an accelerated failure time (AFT) model was constructed. Variable selection for this model was also performed using a stepwise forward and backward selection based on AIC. AFT models are parametric survival models that distribute the probability of failure over time by accelerating or decelerating it among groups. The output estimator for each covariate in these models is the time ratio (TR), which measures how much longer or shorter the time-to-event is on average. The main advantage of AFT models is that they do not rely on the assumption of proportional hazards. All the tests were two-tailed, a p < 0.05 was considered significant. The analyses were performed with R Core Team 2023 (R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria).

Alluvial plot portraying the casualty triage in the study exercise. Note: this alluvial plot visually depicts casualty triage during the study exercise. It shows expected and assigned triage codes at prehospital and in-hospital stages, with stream widths representing casualty numbers. Colours denote triage codes: Green, Yellow, Red, Black, and NA (for unadmitted patients)
Ethics and data protection
Ethical approval was not required as the study focused solely on documenting even frequencies within simulated training programs for learning improvement, with no supplementary interventions conducted. All the authors confirm adhering to the principles outlined in the Declaration of Helsinki while delivering the simulated educational program, ensuring confidentiality. Information stored in the master databases was fully anonymized and was recorded at a group level, due to the inability to associate a particular individual with a specific visited simulator.
Add Comment