


Based on clinical examination including, coughing, tachypnoea, inspiratory dyspnea, nasal discharges, abnormal lung sounds and CRS as well as ultrasonographic findings and postmortem findings for dead and euthanized cases, diseased calves were classified into 4 groups: pulmonary emphysema (n = 8), interstitial pulmonary syndrome (n = 7), bronchopneumonia (n = 12), and pleurisy (n = 8).
Clinical presentation and respiratory score
Clinical presentations were varied according to the respiratory disease condition. At admission, the general condition of most calves was deteriorated. The most observable clinical presentations were dullness, difficult inspiration (mouth breathing, widening of nostrils) (Fig. 1a), and variable degrees of nasal discharges, which was either unilateral or bilateral, that ranged from mucopurulent to purulent in consistency (Fig. 1b). The values of rectal temperature ranged from 38.7 °C to 41 °C. The lowest and highest values of body temperature were noticed in calves with emphysema and pleurisy, respectively. In addition, 8 calves with bronchopneumonia showed pyrexia (mean value of rectal temperature was 40 ± 0.6 °C). The mean value of pulse rate was 92beats/min (range, 78–110). The mean respiratory rate was 43breaths/min (range, 28–52). Upon percussion of the lungs, 5 cases with pulmonary emphysema showed increased and 4 cases with bronchopneumonia had reduced resonance. Upon auscultation of lungs, 3 cases with interstitial pulmonary syndrome exhibited exaggerated vesicular sounds, 5 cases with bronchopneumonia showed moist ráles and 2 cases with pleurisy had pleuritic frictional sounds, resembling two sheets of sandpaper rubbing against each other. Four cases with pulmonary emphysema showed reduced vesicular breath sounds. In contrast, six cases (2 with interstitial pulmonary syndrome and 4 with bronchopneumonia) exhibited no lung sounds by auscultation. The mean values of CRS were significantly higher in all diseased groups in comparison with their corresponding control ones (P < 0.01) (Table 1).

Clinical presentations of calves with respiratory troubles. a Dullness, lacrimation and mouth breathing are signs in a buffalo calf with interstitial pulmonary syndrome (CRS = 5); b ocular secretion (white arrow) and purulent nasal discharges (black arrow) in a cattle calf with bronchopneumonia (CRS = 6). CRS, Clinical respiratory score
Ultrasonographic and postmortem findings
The ultrasonographic appearance of normal aerated lung of control groups was characterized by the uppermost white linear echo, representing parietal and visceral pleurae, with reverberation artifacts (Fig. 2). During respiration, the visceral pleura was seen moving with a real-time examination. Neither lung consolidation nor pleural effusions were visualized in these normal calves. The postmortem examinations of these calves confirmed these ultrasonographic results.

Ultrasonogram of a normal lung generated using a 5 MHz sector probe: hyperechoic pleural line (P) with less echogenic lines parallel to the pleural surface (arrows) represent reverberation artifacts. TW, Thoracic wall; P, Pleura; Ds, Dorsal; Vt, Ventral
In calves with pulmonary emphysema, the ultrasonographic examination of chest showed numerous comet-tail artifacts in the form of bright echogenic bands extending at the lung surface and running perpendicular to the pleura. These comet-tail artifacts ranged from 3 (Fig. 3a) to 4 (Fig. 3b) in number. The most affected lung lobes were the intermediate (5 calves), then the cranial (3 calves) lobes. The Thoracic ultrasonography of buffalo calves with interstitial pulmonary syndrome revealed presence of multiple ultrasound lung comets fanning out from the pleural line to the edge of the image. These lung comets were broader than that in emphysema and the entire ultrasound image appeared white in colour (Fig. 4a). At postmortem examinations of these calves, their lungs were severely congested and edematous (Fig. 4 b).

Ultrasonograms of the lung of buffalo calves with pulmonary emphysema. a A mild case of pulmonary emphysema shows few echogenic bands (C) run from the lung surface with reverberation artifacts (arrows); b A severe case of pulmonary emphysema shows multiple echogenic bands (C) originate from the pleural surface. TW, Thoracic wall; P, Pleura; Ds, Dorsal; Vt, Ventral; C, Comet-tail artifacts

Ultrasonogram and postmortem finding of a buffalo calf with interstitial pulmonary syndrome. Image (a) shows multiple ultrasound lung comets fanning out from the pleural line to the edge of the image (arrows), white lung. Image (b) represents postmortem findings of the same calf that shows severely congested and edematous lung. TW, Thoracic wall; P, Pleura; Ds, Dorsal; Vt, Ventral; RS, Rib shadowing
In calves with bronchopneumonia, the ultrasonographic appearance of diseased lungs varied depending on the degree and type of lesions. Four cases showed small hypoechoic circular zones (about 7 mm in diameter) at the lung surface, representing a superficial fluid alveologram with a comet-tail artifact (Fig. 5a). The ultrasonographic features of the lung tissue in ten calves with bronchopneumonia appeared hypoechoic and its echo texture may look like liver parenchyma, representing pulmonary consolidation and containing ramified fluid bronchgrams (Fig. 5b). These consolidated areas have a homogenous and echoic basic texture with well defined borders. Lesions of lung consolidation were found on the left side of the thorax in 7 cases and on the right side of the thorax in 3 cases. In three cases, air-filled alveoli were imaged in this hepatized lung tissue, appearing as hyperechoic spots in the consolidated parenchyma. Occasionally, hyperechoic reflective bands of an air-filled bronchus were detected in the pulmonary tissue, representing air bronchoaerograms. The most affected lobes were the cranial (8 calves) (Fig. 5c), then the cardiac (2 calves) and intermediate (2 calves) lobes. Thoracic ultrasonographic examination of calves with pleurisy revealed presence of thick fragmented visceral pleura and filling of pleural sac with echogenic fibrin shreds and anechoic exudates (Fig. 6). Moderate pleural effusion was seen in 3 cases, while pleural irregularity was observed in 4 of 8 cattle calves with pleurisy. One case showed roughened texture of the pleural surface causing narrow streaks of comet tails.

Ultrasonograms of cattle calves with bronchopneumonia. a An image for a mild case shows a small hypoechoic zone on the surface of the lung (arrow, diameter: 7 mm), representing fluid alveologram with comet-tail artifact (C). b An image for the cranial lobe of a severely bronchopneumonic calf shows consolidated lung with ramified fluid bronchograms (FG). c This image represents postmortem findings of the same case in image B showing consolidation of the cranial lobe (arrow). TW, Thoracic wall; P, Pleura; Ds, Dorsal; Vt, Ventral; CL, Consolidated lung

Ultrasonogram of a lung of cattle calf with fibrinous pleurisy exhibits interrupted visceral pleura (VP) with accumulation of fibrin (F) and inflammatory exudates forming pleural effusion (PE). TW, Thoracic wall; Ds, Dorsal; Vt, Ventral; L, Lung
Pearson’s correlation coefficients were calculated to find the relationship between ULS and CRS. A weak correlation was noticed between the two variables (r = 0.55, P < 0.01) (Fig. 7).
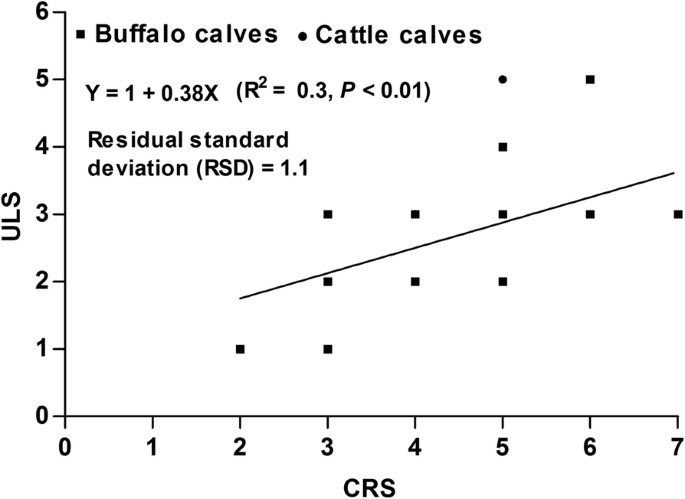
A scatter plot for the relationship between the clinical respiratory scores (CRS) and ultrasound lung scores (ULS) in calves with respiratory troubles
Hematological and biochemical findings
Table 2 summarizes the mean values of hematological and biochemical indices in calves with respiratory troubles. The total white blood cell counts were higher in all diseased groups in comparison with the corresponding controls (P < 0.05). The mean values of serum total proteins and globulins were significantly increased only in calves with bronchopneumonia (P < 0.05). The serum activities of AST were higher in buffalo claves with emphysema and interstitial pulmonary syndrome in comparison with the corresponding control group (P < 0.05). Arterial blood gas analysis revealed increased partial tension of carbon dioxide (PCO2) in all diseased. In contrast, the mean values of partial tension of oxygen (PO2) were decreased in all diseased groups (P < 0.05).
The association between the laboratory parameters and various respiratory troubles is summarized in Table 3 for 26 calves with ultrasound lung score ≥ 1 and clinical respiratory score ≥ 5. It was noticed that only WBCs and PCO2 were significantly (P = 0.006) and (P = 0.004), respectively, indicated respiratory troubles in weaned calves. However, weak correlations were observed between ULS and WBCs (r = 0.47, P < 0.1) and ULS and PCO2 (r = 0.36, P < 0.05) (Table 4).
Therapy and outcome
Calves were treated with 8.7 mg/kg amoxicillin trihydrate, clavulanic acid (Synulox®) injected once daily into the muscles of the neck or hindquarters. Bromhexine Hydrochloride (Bisolvon) in a dose 0.5 mg/kg per os. 0.5 mg/kg meloxicam (metacam) intravenous injection. The clinical signs including CRS and appetite were improved in most diseased calves, therefore; they were discharged from the hospital one or 3 days after beginning of treatment and the importance of completing the therapeutic course was emphasized to the owner and referring veterinarian.
Ten cattle calves with bronchopneumonia were severely diseased and they kept in the hospital for a month and examined clinically and ultrasonographically for assessment of therapy. After 3 days from the beginning of treatment, coughing and nasal discharges were much reduced. The clinical respiratory score was improved after 5 days (Table 5). Few crackle sounds were heard over lung lesion. Crackles were not consistently identified in 6 calves despite the presence of lung hepatization noted during ultrasonographic examination. Follow-up ultrasound examination of calves revealed gradual improvement and tissue healing (Fig. 8). One incurable case was euthanased and sent for necropsy examination, which revealed gross lung pathology and exudation.
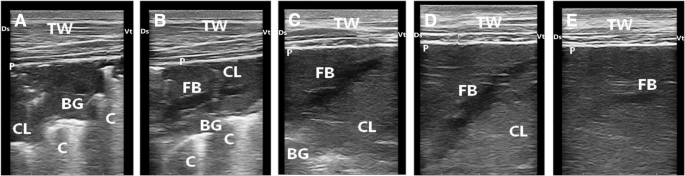
Ultrasonograms of a calf with severe bronchopneumonia show the development of pulmonary lesions during the course of therapy. Image (a), at admission of the calf, reveals consolidated cranial lobe (CL) with hyperechoic bronchoaerogram (BG). Image (b) for the same calf after 5 days of therapy shows consolidated cranial lobe (CL), bronchoaerogram (BG) and fluid bronchogram (FB). Image (c), after 10 days of therapy, exhibits consolidated lung (CL) and few bronchoaerograms (BG). Image (d), after 20 days of therapy, reveals improvement of pulmonary lesions but lung consolidation (CL) and fluid bronchogram (FB) are still present. Image (e), after 30 days of therapy, shows an obvious improvement in the pulmonary tissue in comparison with previous images but a remnant of fluid bronchogram (FB) is still present. TW, Thoracic wall; P, Pleura; Ds, Dorsal; Vt, Ventral
Add Comment